Cornell note:
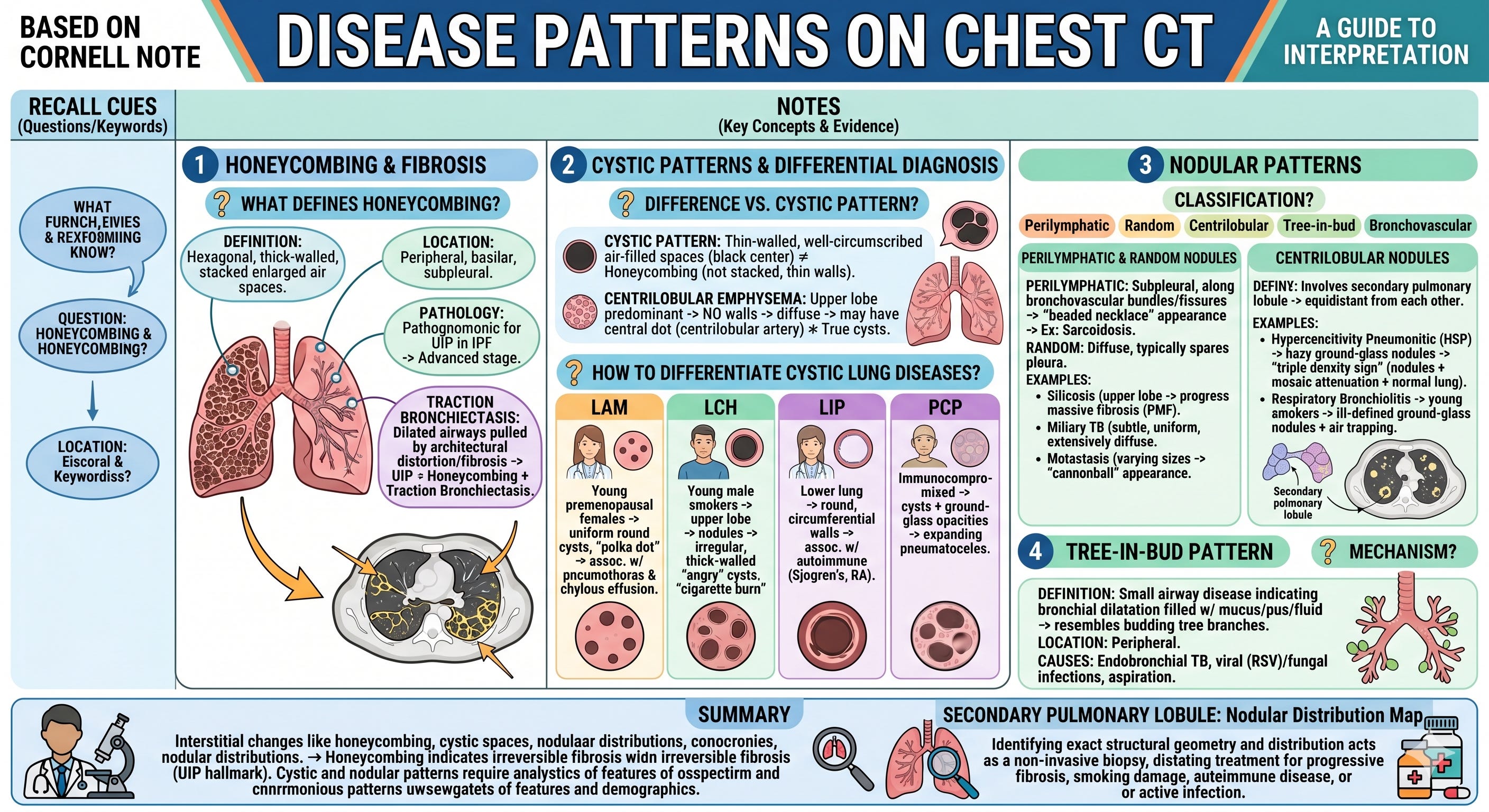
What defines “Honeycombing”?
Definition: Hexagonal, thick-walled, stacked enlarged air spaces.
Location: Peripheral, basilar, subpleural.
Pathology: Pathognomonic for UIP (Usual Interstitial Pneumonia) in IPF (Idiopathic Pulmonary Fibrosis) → signifies advanced stage.
Traction Bronchiectasis: Dilated airways pulled by architectural distortion/fibrosis → UIP = Honeycombing + Traction Bronchiectasis
Difference vs “Cystic Pattern”?
Cystic Pattern: Thin-walled, well-circumscribed air-filled spaces (black center) ≠ Honeycombing (not stacked, thin walls).
Centrilobular Emphysema: Upper lobe predominant → NO walls → diffuse → may have central dot (centrilobular artery) ≠ True cysts.
How to differentiate Cystic Lung Diseases?
LAM (Lymphangioleiomyomatosis): Young premenopausal females → uniform round cysts surrounded by normal lung (”polka dot”) → assoc. w/ pneumothorax & chylous effusion.
LCH (Langerhans Cell Histiocytosis): Young male smokers → upper lobe → nodules → irregular, thick-walled “angry” cysts (”cigarette burn”).
LIP (Lymphocytic Interstitial Pneumonia): Lower lung → round, circumferential walls → assoc. w/ autoimmune (Sjogren’s, RA).
PCP (Pneumocystis Pneumonia): Immunocompromised → cysts + ground-glass opacities → expanding pneumatoceles.
“Nodular Patterns” classification?
Based on distribution: Perilymphatic, Random, Centrilobular, Tree-in-bud, Bronchovascular.
Characteristics of “Perilymphatic” & “Random”Nodules?
Perilymphatic: Subpleural, along bronchovascular bundles/fissures → “beaded necklace” appearance → Ex: Sarcoidosis.
Random: Diffuse, typically spares pleura.
Ex 1: Silicosis → upper lobe → coalesces into progressive massive fibrosis (PMF).
Ex 2: Miliary TB → subtle, uniform, extensively diffuse.
Ex 3: Metastasis → varying sizes → “cannonball” appearance.
Characteristics of “Centrilobular” Nodules?
Definition: Involves secondary pulmonary lobule → equidistant from each other.
Ex 1: Hypersensitivity Pneumonitis (HSP) → hazy ground-glass nodules → “triple density sign” (nodules + mosaic attenuation + normal lung).
Ex 2: Respiratory Bronchiolitis → young smokers → ill-defined ground-glass nodules + air trapping.
Mechanism of “Tree-in-Bud” pattern?
Definition: Small airway disease indicating bronchial dilatation filled w/ mucus/pus/fluid → resembles budding tree branches.
Location: Peripheral.
Causes: Endobronchial TB, viral (RSV)/fungal infections, aspiration.
Summary:
Chest CT disease patterns can be broadly categorized into interstitial changes like honeycombing, cystic spaces, and distinct nodular distributions. Honeycombing indicates irreversible fibrosis and is the hallmark of Usual Interstitial Pneumonia (UIP). Conversely, cystic and nodular patterns require careful analysis of wall thickness, anatomical distribution (upper vs. lower, perilymphatic vs. random), and patient demographics to narrow down the differential diagnosis accurately.
Significance: Identifying the exact structural geometry and distribution of lung opacities on a CT scan acts as a non-invasive biopsy, directly dictating whether the clinician treats for progressive fibrosis, smoking-related damage, autoimmune disease, or active infection.